Episode 76 Pediatric Procedural Sedation
- Author
- Dr. Anton Helman
- Published
- Tue 09 Feb 2016
- Episode Link
- https://emergencymedicinecases.com/pediatric-procedural-sedation/
In this EM Cases episode on Pediatric Procedural Sedation with Dr. Amy Drendel, a world leader in pediatric pain management and procedural sedation research, we discuss how best to manage pain and anxiety in three situations in the ED: the child with a painful fracture, the child who requires imaging in the radiology department and the child who requires a lumbar puncture. Without a solid understanding and knowledge of the various options available to you for high quality procedural sedation, you inevitably get left with a screaming suffering child, upset and angry parents and endless frustration for you. It can make or break an ED shift. With finesse and expertise, Dr. Drendel answers such questions as: What are the risk factors for a failed Pediatric Procedural Sedation? Why is IV Ketamine preferred over IM Ketamine? In what situations is Nitrous Oxide an ideal sedative? How long does a child need to be observed in the ED after Procedural Sedation? Do children need to have fasted before procedural sedation? What is the anxiolytic of choice for children requiring a CT scan? and many more...
Written Summary & blog post by Michael Kilian, edited by Anton Helman, February 2016
Cite this podcast as: Drendel, A, Helman, A. Pediatric Procedural Sedation. Emergency Medicine Cases. February, 2016. https://emergencymedicinecases.com/pediatric-procedural-sedation/. Accessed [date].
This Pediatric Procedural Sedation episode is paired with Episode 67 Pediatric Pain Management
Bridging Analgesics: Triage to Procedural Sedation
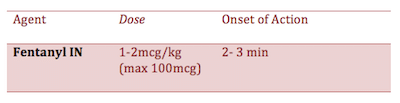
Your initial approach to pain control when the patient hits the ED door will depend on severity of pain. For presentations of severe pain, intranasal fentanyl is a recommended first line agent as it is fast and easy to administer, avoids requiring cooperation with oral medications, and provides reliable analgesia that has been shown to be equivalent to intravenous morphine. For mild to moderate pain, consider oral agents such as ibuprofen, which has been shown to be more effective than acetominophen for pain control in orthopedic injuries in children.
Intranasal (IN) Fentanyl
A general rule of thumb for dosing IN fentanyl is twice the IV dose.
Tips to increase your success with intranasal fentanyl and other IN medications:
* Avoid intranasal medications in children with obviously congested nares since absorption will decrease and dosing will be unreliable
* Choose the highest concentration formulation of fentanyl as this will allow you to use a smaller volume
* Use BOTH nostrils for volumes over 0.3 ml to double the absorptive surface and reduces runoff
* Consider administering an oral analgesic concurrently for continued pain management after the Fentanyl has worn off
* Respiratory depression is rare with correct dosing, however naloxone is also effective intranasally, if needed, as a reversal agent
* Instruct the child to take deep breath in “like smelling a flower”
For guidance around use of intranasal medications we recommend www.intranasal.net. This resource provides evidence-based recommendations for a variety of applications of intranasal medication including pain control, sedation and seizure management.
Distraction Techniques for Pediatric Procedural Sedation
There is good evidence to support the use of distraction techniques to help decrease the child’s anxiety and pain experience during a procedure. Familiar faces and various technological devices such as smartphones and tablets may be effective at calmin...

{kind=link}