Episode 67 Pediatric Pain Management
- Author
- Dr. Anton Helman
- Published
- Tue 07 Jul 2015
- Episode Link
- https://emergencymedicinecases.com/pediatric-pain-management/
Pain is the most common reason for seeking health care. It accounts for 80% of ED visits. The WHO has declared that “optimal pain treatment is a human right”. As has been shown in multiple ED-based Pediatric pain management studies, Pediatric pain is all too often under-estimated and under-treated. Why does this matter? Under-estimating and under-treating pediatric pain may have not only short term detrimental effects but life-long detrimental effects as well; not to mention, screaming miserable children disturbing other patients in your ED and complaints to the hospital from parents. Whether it’s venipuncture, laceration repair, belly pain or reduction of a fracture we need to have the skills and knowledge to optimize efficient and effective pain management in all the kids we see in the ED. What are the indications for intranasal fentanyl? intranasal ketamine? Why should codeine be contra-indicated in children? How do triage-initaited pain protocols improve pediatric pain management? Which are most effective skin analgesics for venipuncture? To help you make these important pediatric pain management decisions, in this podcast we have one of the most prominent North American researchers and experts in Emergency Pediatric pain management, Dr. Samina Ali and not only the chief of McMaster Children’s ED but also the head of the division of Pediatric EM at McMaster University, Dr. Anthony Crocco.
Written Summary and blog post prepared and written by Dr. Anton Helman, July 2015
Cite this podcast as: Helman, A, Ali, S, Crocco, A. Pediatric Pain Management. Emergency Medicine Cases. July, 2015. https://emergencymedicinecases.com/pediatric-pain-management/. Accessed [date].
Why is Pediatric Pain Management Important?
Short-term detrimental effects of painful procedures
* Extended procedure duration and length of stay
* Slower surgical healing
* Emotional trauma and suffering
Long-term detrimental effects of painful procedures
* Infant pain may actually change pain processing
* Avoidance/heightened sensitivity to medical care
* Fear/increased pain experienced healthcare evaluation
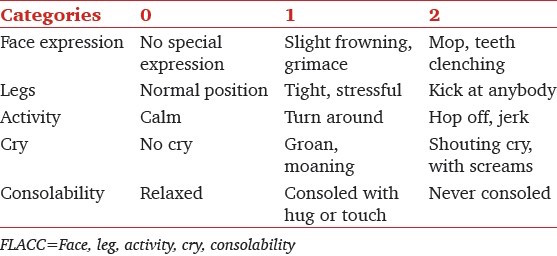
Pediatric Pain Assessment Tools
A) Infants
FLACC Scale (out of a total score of 10)
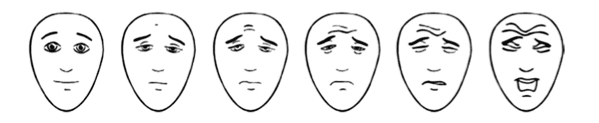
B) 4-8 years old
Faces Pain Scale Revised (child points to face that best describes their pain)
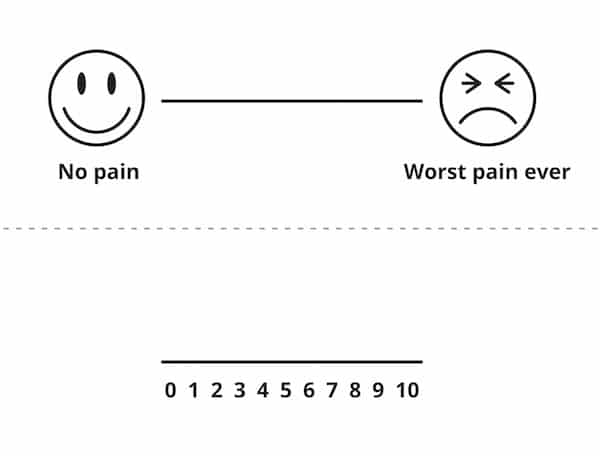
C) 8-15 years old
Visual Analog Scale
Do vital signs help in Pediatric Pain Assessment?
There is no correlation between improvement in pain scores and changes in heart rate, respiratory rate or blood pressure. Using vital signs to assess pain in children may be misleading.
Triage-Initiated Pain Protocols
A nurse-driven protocol at triage has been shown to improve time-to-analgesia. Many Canadian hospitals employ oral acetaminophen or ibuprophen triage-initiated pain protocols, and some in Canada and Australia employ intranasal fentanyl and oral opiods.
Low Resource Utilization Distraction Techniques
Infants
* Breastfeeding or breast milk has been shown to temper pain but has not been established for repeated painful procedures
* Oral Sucrose (2mL) reduces signs of distress in infants when given 2 minutes before the procedure and the analgesic effect can be augmented with non-nutritive sucking via a pacifier. If oral sucrose is not available,

{kind=link}
{kind=link}
{kind=link}